News Update: What You Need to Know About the Court Case Attacking Access to Mifepristone in the United States


The right to appropriate, acceptable and affordable health care is guaranteed to all under Zimbabwe’s constitution. This commitment to universal health coverage — outlined in the 2016-2020 national health strategy — derives from the government’s adoption of a primary health care approach in 1984. However, the core principles of primary health care have since been hampered by fiscal and environmental challenges. To strengthen the foundation of the country’s health system, Zimbabwean health advocates are working with communities to claim their rights guaranteed by the government.
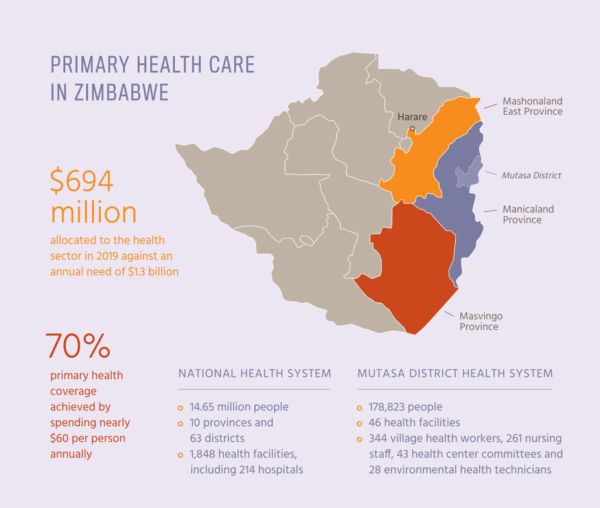
Primary health care is a people-centered, comprehensive approach that aims to increase access and availability of care in addition to supporting community participation in the health system. Although primary health care has brought facilities and health workers closer to underserved areas, community-based services receive less than 15% of the national health budget. In the Manicaland, Masvingo and Mashonaland East provinces, natural crises such as Cyclone Idai and drought have magnified the impact of health sector strikes protesting inadequate salaries and persistent lack of supplies and functional infrastructure.
Despite underinvestment, Zimbabwe’s community health systems are supported by local efforts to mobilize funding and improve the quality of service provision. Since 1998, a network of civic- and community-based organizations, the Community Working Group on Health (CWGH), has been leading the movement to secure equitable health services by enhancing community involvement in health planning, budgeting and accountability in all 10 provinces.

CWGH advocates at the central level for sufficient public funding of community health services and staff — including nurses, village health workers and environmental health technicians — and structures for local engagement, specifically health center committees. By resourcing health literacy and capacity development for communities, the government can sustain these strategies to bolster social accountability and local participation in health throughout Zimbabwe.

In the Mutasa district of Manicaland province, people seeking health services must travel between 12 to 50 kilometers to reach the nearest facility. For its farming communities like Stapleford Estate, most privately owned clinics have closed over the past decade due to incapacitation, and community members have since relied on traditional and herbal medicine. To achieve universal health coverage, CWGH is advocating for the government to reopen and run these facilities to improve access to care.



The Sakupwanya Clinic is a public facility in this rural community serving over 5,000 people across 25 villages. The partnership among its nurses and the district village health workers, environmental health technicians and health center committees illustrates the principles of sustainable, quality, equitable and community-led primary health care — and the urgency of strengthened government support.

Each year, the Sakupwanya Clinic submits detailed funding requests to the central government. However, due in part to lack of funds, there is low government recruitment of staff and the clinic doesn’t receive much of the money needed for operations. As a supplement to public health funds, Sakupwanya Clinic is supported by results-based financing, which stipulates that certain health provision goals must be met in order to receive aid. This development approach temporarily fills funding gaps in services and supplies by requiring nurses who are already overworked to meet various indicators.


At the Sakupwanya Clinic, this program has financed new infrastructure for patients waiting to access health services, essential medicines and equipment. Despite these short-term improvements, the community health system has been weakened overall. Performance-based targets identified by donors are often approved and implemented by the government without engaging providers and civil society — creating incentives which are ultimately unresponsive to local health needs and expectations.

The sister-in-charge at Sakupwanya Clinic, Sr. Patience Chindondondo, goes beyond prescribed incentives to build trust with the community — a key component of quality in a primary health care setting. Every morning, she and her staff host health talks to raise awareness and tackle misinformation on topics like family planning. For nurses at the clinic, like Sr. Shylet Putsai, these opportunities to engage with patients offer motivation despite low wages.
“I enjoy my work and feel encouraged especially when people thank me and show gratitude for helping them when they come to the clinic.”


To complement these community health education sessions, the clinic staff works with environmental health technicians to improve service quality. Technicians train Mutasa district’s nurses, village health workers and health center committee members on how to maintain a safe and hygienic environment to prevent the spread of disease — particularly during crises like Cyclone Idai. Rejoyce Kasererah, who serves as an environmental health technician intern, assists with keeping the community up to date on public health announcements and connecting local providers and advocates to the government.

Geographic distance and fear of discrimination can be major drivers of health inequity. Under Sr. Patience’s supervision, village health workers, like Shandukurai Fombe, host discussions on issues such as early childhood stimulation at the clinic to strengthen relationships with the community. Becoming known as a familiar, trusted provider offers Shandukurai the opportunity to reach more people when she conducts home visits. These visits are critical to ensure that members of the community unable or unwilling to seek care at the clinic — due to accessibility challenges such as transportation costs or social barriers like stigma facing those living with HIV and AIDS — are not overlooked by the health system.


Shandukurai lives in Mandianike village and delivers care to households as far as 18 kilometers away. During home visits, she is responsible for treating common conditions, referring more complex cases to the appropriate facility and promoting healthy behaviors, such as immunization. Shandukurai receives a modest quarterly allowance from the government, but often, that payment isn’t sent in a timely manner and she must use her own resources to continue working.
“There is nothing much I get as incentives,” says Shandukurai. “Instead, I work for the passion of saving lives.”

Health center committees, with support from CWGH, strengthen the primary health care system’s connection to the communities it serves. When there are stockouts of essential medicines or long wait times to receive care, these committees host conversations between patients and providers to resolve misunderstandings and work together on solutions. To improve water and sanitation services, the health center committee at Stapleford Estate advocates for the reopening of the community’s closed facility, health outreach through a mobile clinic, restored reservoir tanks and increased water points from the government.


At the Sakupwanya Clinic, the health center committee meets with Sr. Patience and her staff to discuss community concerns and make contributions to the facility’s operational plans and budgets, as well as service quality. Where possible, the committee pools resources to compensate for shortfalls in the primary health care budget — successfully funding projects like a new maternity wing. These initiatives have brought together the community, including its traditional leadership, and supported local demands for better health outcomes.

These stories from Manicaland province illustrate that local providers and communities are taking action to ensure equitable coverage and to navigate the mistrust that has manifested with underinvestment of the health sector. The health center committees in Mutasa district — in partnership with clinic staff, environmental health technicians and village health workers — are making strides to mobilize the community around their right to quality health care.
CWGH has supported these health center committees to monitor the primary health care budget and advocate for increased funding. In addition to equipping committee members with tools to engage government officials, CWGH has developed guidelines detailing their roles and successfully advocated for legal recognition of health center committees under the 2018 Public Health Act.
By implementing these policies, the Ministry of Health and Child Care can more effectively support community participation and achieve a sustainable, people-centered health system in Zimbabwe. CWGH will continue to advocate on behalf of health center committee members to ensure that these local leaders are democratically elected, represent the diversity in their districts and receive the necessary information and training to better serve their communities.
The Ministry of Health and Child Care has been a CWGH partner in the advocacy and social accountability work being implemented in the Mutasa district and Manicaland province.

We are fighting back against the onslaught of harmful policies that discard reproductive rights.
Stay informed about the issues impacting sexual and reproductive health and rights.

