Purpose
Continuing a PAI effort begun in 1995, the Reproductive Health Index is the fifth in a series of reports assessing the status of nations’ sexual and reproductive health and rights (SRHR). While our previous indices frame the issues in terms of sexual and reproductive risk, this iteration deliberately shifts its focus to how to achieve healthy sexual and reproductive health and realize rights.
The aim is to provide an assessment that incorporates a multi-dimensional approach to reproductive health and adds a new perspective to how comprehensive SRHR is defined and measured. The Index and its accompanying report provide a measure of where women in 62 low- and lower-middle-income countries stand in attaining sexual and reproductive health and rights.
A country’s Index score aggregates key dimensions of SRHR into a summary measure of achievement. This summary measure offers a simple and direct way to: understand a larger and more complex set of issues, guide investments, measure progress and spur appropriate action. Accordingly, the Index serves as a catalyst for dialogue and action among policymakers, program designers, program implementers, advocates and donors alike.
The Index provides a snapshot of the status of women’s SRHR in each country and allows stakeholders to see how countries compare to one another. The Index also provides insight on where gaps exist and, consequently, where there are opportunities for targeted attention and investment. Strengths and weaknesses among regions and countries can serve as driving forces of change. A country’s Index score can also serve as a reference point to assess how well government investments, policies and programs are meeting the needs of women.
It is important to note that while indicators and indices are valuable tools for broad analysis, they cannot measure the full scope of any one issue. A fuller picture of women’s SRHR status requires additional analysis. Accordingly, the chapters of our report provide a more in-depth look at the dimensions of SRHR and provide analysis of information beyond the indicators used to construct the Index.
Methodology
Based on the 1994 Programme of Action of the International Conference on Population and Development, we define SRHR according to the following four dimensions:
-
Preventing unintended pregnancy;
-
Increasing access to safe abortion and post-abortion care;
-
Helping women safely through pregnancy, childbirth and the postpartum period; and
-
Preventing and treating sexually transmitted infections, including HIV/AIDS.
A fifth dimension, termed the “enabling environment,” captures factors beyond the health system that support sexual and reproductive health and rights.
Rather than measuring the health outcomes corresponding to the dimensions noted above, this Index captures the factors driving the attainment of SRHR. Determinants include access to high-quality, voluntary and affordable health services and supplies; high-quality information; and non-restrictive and non-coercive laws and policies.
To calculate an Index score for each country, 11 indicators representing the dimensions of SRHR were combined into a single measure—the Reproductive Health Index. To view the list of indicators and a full description of how the Index was constructed, please see the report Methodology.
The Index is scored on a 0 to 100 scale. Therefore, the strongest possible state of SRHR in a country according to the Index would be a score of 100.
Findings
Index scores for the 62 countries included in our study range from 25.5 to 86.5. Though scores vary greatly within that range, the fact that no country received a score of 100 means that there are opportunities to advance the sexual and reproductive health and rights of women in all 62 countries.
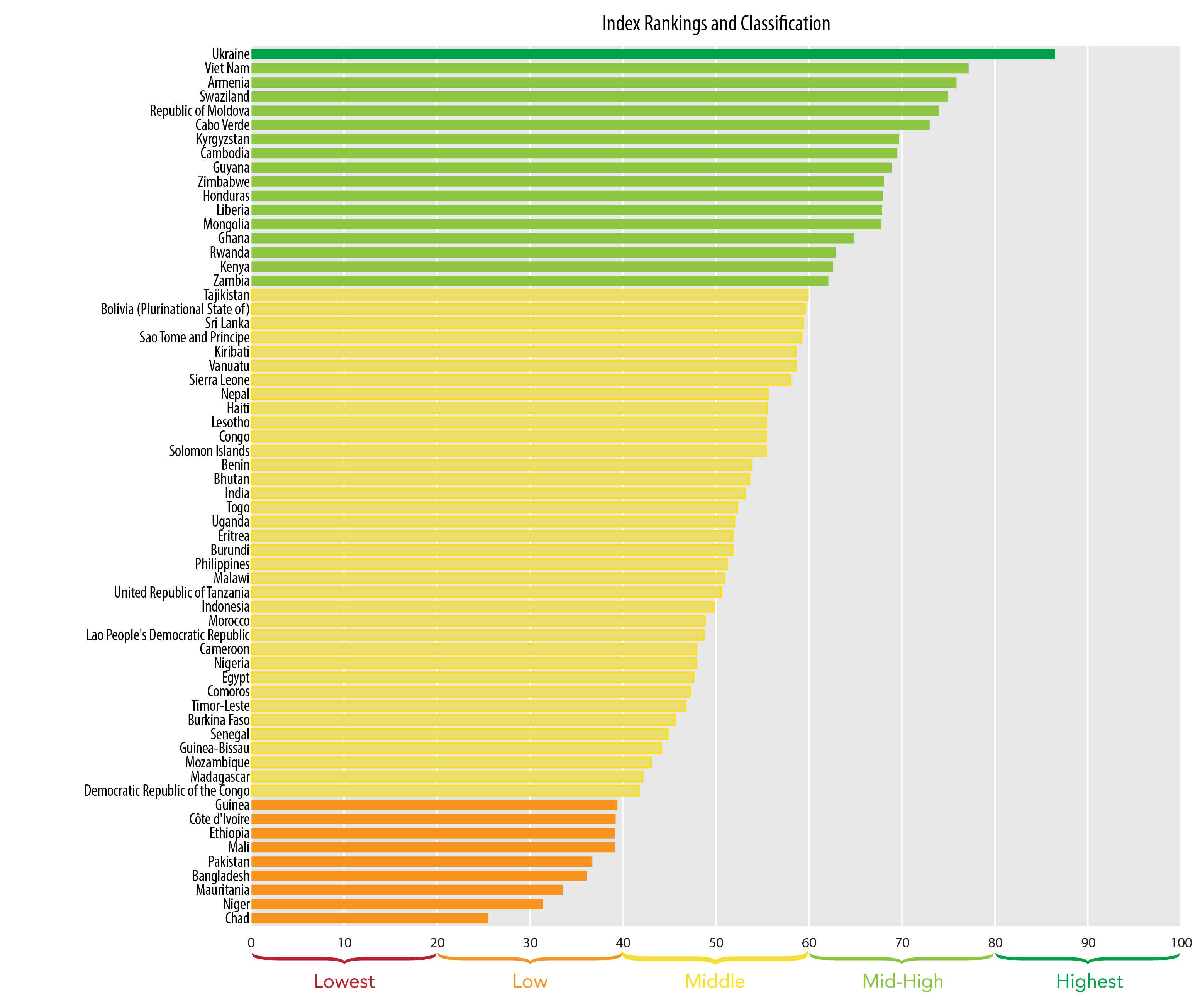
HIGHEST CATEGORY (Index scores 80 to 100)
1 country
Ukraine, a lower-middle-income country, is the only nation with an Index score higher than 80. According to World Bank estimates, this Eastern European country’s gross national income (GNI) per capita has risen by $460 from $3,500 in 2012 to $3,960 in 2013. This puts Ukraine’s GNI per capita $165 away from being an upper-middle-income country. Indicators for Ukraine demonstrate that:
- Ninety-three percent of women in Ukraine have their demand for contraception satisfied and 82 percent of women were able to make an informed choice about their contraceptive method as a result of the information they received from their health care providers.
- Ukraine does not place policy restrictions on abortions. This means under Ukraine’s legal framework, women can choose to have an abortion without restriction as to reason.
- A high percentage of women in Ukraine are reported to receive at least four antenatal visits during their pregnancies and almost 99 percent of births are attended by skilled health personnel.
- More than 90 percent of women demonstrate comprehensive knowledge of HIV prevention methods. However, less than half of the women eligible for antiretroviral therapy are receiving treatment.
- Indicators representing an enabling environment were high for women in Ukraine. Most women (more than 90 percent) were not married as children or adolescents and almost 88 percent of married women participate in all household decisions either alone or jointly with their husbands.
MID-HIGH CATEGORY (Index scores 60 to 79)
16 countries
Countries in this category are regionally diverse, with Asia, Europe, Latin America and the Caribbean, and Africa all represented. The majority of countries in this category are lower-middle-income countries.
- Data show that an average of 71 percent of women in these countries have their demand for contraception satisfied. However, Ghana and Liberia are outliers, as less than 40 percent of women had their demand satisfied in these countries. An average of nearly 58 percent of women in this category were able to make an informed choice about their contraceptive method as a result of the information they received from their health care providers. However, the ability of women to make an informed choice in Cabo Verde and Mongolia is below 35 percent.
- Abortion is legal under some circumstances in all but one country in this category; in Honduras, abortion is prohibited. In eight of the 16 countries, abortion is permitted without restriction as to reason. Additionally, 11 out of the 16 countries have misoprostol (a drug that can be used to effectively treat certain complications from unsafe abortion) listed on their Essential Medicine Lists.
- The majority of women in these countries report receiving at least four antenatal visits during their pregnancies, except in Rwanda and Kenya, where antenatal coverage is below 50 percent. The majority of births (close to 80 percent) are attended by skilled health personnel, with the exceptions of Kenya and Zambia, where skilled birth attendance is less than 47 percent.
- The percentage of women with an STI or potential STI symptoms who sought advice or treatment from a health professional is less than 64 percent on average. Generally, women in these countries demonstrate a high level of knowledge of HIV prevention, and an average of 71 percent of women eligible for anti-retroviral therapy are receiving treatment. However, antiretroviral coverage is notably low in Moldova, Mongolia and Liberia.
- Enabling environment indicators reveal an average of 80 percent of women were not married as children or adolescents and 64 percent of married women participate in all household decisions either alone or jointly with their husbands. Household decision-making is particularly low in the sub-Saharan African nations of Swaziland, Cabo Verde, Ghana and Zambia.
MIDDLE CATEGORY (Index scores 40 to 59)
36 countries
Twenty of the 36 countries in this category are from sub-Saharan Africa. There is a near equal split of low- and lower-middle-income countries in this group.
- An average of 57 percent of women in these countries have their demand for contraception satisfied and an average of 57 percent of women in this category were able to make an informed choice about their contraceptive method as a result of information they received from their health care providers.
- Abortion is legal under some circumstances in 26 countries in this category, two of which allow abortion without restriction as to reason. Abortion is prohibited altogether in ten of the countries in this category. Just over half of the 27 countries in this group have misoprostol (a drug that can be used to effectively treat certain complications from unsafe abortion) listed on their Essential Medicine Lists.
- Approximately 59 percent of women in these countries report receiving at least four antenatal visits during their pregnancies, and 63 percent of births are attended by skilled health personnel.
- The percentage of women with an STI or potential STI symptoms who sought advice or treatment from a health professional is 54 percent on average. Fifty-seven percent of women in these countries demonstrate a high level of knowledge of HIV prevention, and less than half of women eligible for antiretroviral therapy are receiving treatment. Antiretroviral coverage is as low as one percent in Madagascar.
- Enabling environment indicators reveal that 70 percent of women were not married as children or adolescents, and only 46 percent of married women participate in all household decisions either alone or jointly with their husbands. Household decision-making is particularly low in the sub-Saharan African nations of Malawi, Cameroon, Burkina Faso and Senegal.
LOW CATEGORY (Index scores 20 to 39)
9 countries
The majority of countries in this category are low-income countries in sub-Saharan Africa. With the exception of a few outliers, indicators for these countries are low on both health and the overall enabling environment.
- An average of only 41 percent of women in these countries have their demand for contraception satisfied, and an average of less than 37 percent of women in this category were able to make an informed choice about their contraceptive method as a result of information they received from their health care providers.
- Abortion is legal under some circumstances in eight countries, but none allow abortion without restriction as to reason. Abortion is prohibited altogether in one country—Mauritania. Only three countries in this group have misoprostol listed on their Essential Medicine Lists.
- Just over a third of women in these countries report receiving at least four antenatal visits during their pregnancies, and less than half of births (41 percent) are attended by skilled health personnel.
- The percentage of women with an STI or potential STI symptoms who sought advice or treatment from a health professional is less than 39 percent on average. Close to 41 percent of women in these countries demonstrate a high level of knowledge of HIV prevention, and less than half of women eligible for antiretroviral therapy are receiving treatment.
- Enabling environment indicators reveal less than half of women were not married as children or adolescents, and only 29 percent of married women participate in all household decisions either alone or jointly with their husbands. Household decision-making is particularly low in the sub-Saharan African nations of Mali and Niger.
LOWEST CATEGORY (Index scores 0 to 19)
0 countries
Thankfully, no countries had Index scores that fell within the lowest possible range.
Recommendations
The Index findings demonstrate the need for greater investment in, and targeted attention to, fulfilling the SRHR of women in all countries included in the Index. Accordingly, there is a need to go beyond rhetorical commitment to real action for SRHR. SRHR must be considered an integral component of any health systems strengthening approaches. Women and men, boys and girls face a variety of SRHS needs over the course of their lifetimes. Reproductive health should no longer be a siloed health consideration but rather should be addressed as a foundational aspect of overall health and well-being.
Though gaps in meeting the needs and fulfilling the rights of women may be larger in some countries than others, even those countries with higher scores have room to grow. Our analysis indicates that improving the SRHR of women in these countries depends on three overarching actions:
- Strengthen political will and financial commitments: At the national level, family planning and reproductive health programs with high-level political support and sustainable financial resources are more successful. This type of leadership and commitment are critical to ensuring that policies promote meaningful access to contraceptives, resources are made available, and reproductive health programs are prioritized.
- Craft and implement positive policies: There remains a need to go beyond eliminating policy barriers related to sexual and reproductive health information, services and supplies. Policies need to champion individual reproductive rights, including among historically disadvantaged and marginalized populations. For example, women’s reproductive autonomy should be ensured beyond simply eliminating spousal and parental consent regulations. The reproductive health needs of youth must be openly acknowledged in policies and youth-friendly services need to be prioritized and integrated within existing programs.
- Provide quality information and services: Attention is often centered on attracting new contraceptive users to increase contraceptive prevalence rates. However, investing in high-quality information, services and supplies is critical for meeting the needs of current users. Preventing unintended pregnancies depends upon sustaining satisfied contraceptive users, not simply acceptors. This requires greater emphasis on quality information, counseling and overall service delivery that meets the needs of women throughout their reproductive lives.


